Read the following case study and answer the questions that follow. Most os the terms are included in this chapter. Refer to the Glossary or to your medical dictionary for the other terms.
Chronic Obstructive Pulmonary Disease (COPD)
Helga Freiderick is a 57 year-old woman who came to the urgent care clinic today complaining of SOB. On admission, her respirations were labored at a rate of 32. Her Spo2, was just 84%, and her VC was decreased. She appeared anxious and stated that she “couldn’t get enough air.” Her lungs had bilateral expiratory wheezes throughout, scattered rhonchi, and bibasilar crackles. She had a frequent cough productive of thick green sputum.
Stat ABG were drawn, she was put on O2 at 2 lpm per NC and given a nebulizer Tx. A sputum specimen was collected and sent for C and S. She was given IV doses of a broad spectrum antibiotic and a steroid drug. Upon review of her ABGs, it was determined that she was in a state of mild respiratory acidosis.
A short time later, Mrs. Freidericks’ respiratory rate had decreased to 20, her O2 saturation was 91%, and she stated that she was breathing “much better.” She was then transferred to the hospital for further monitoring and continued therapy.
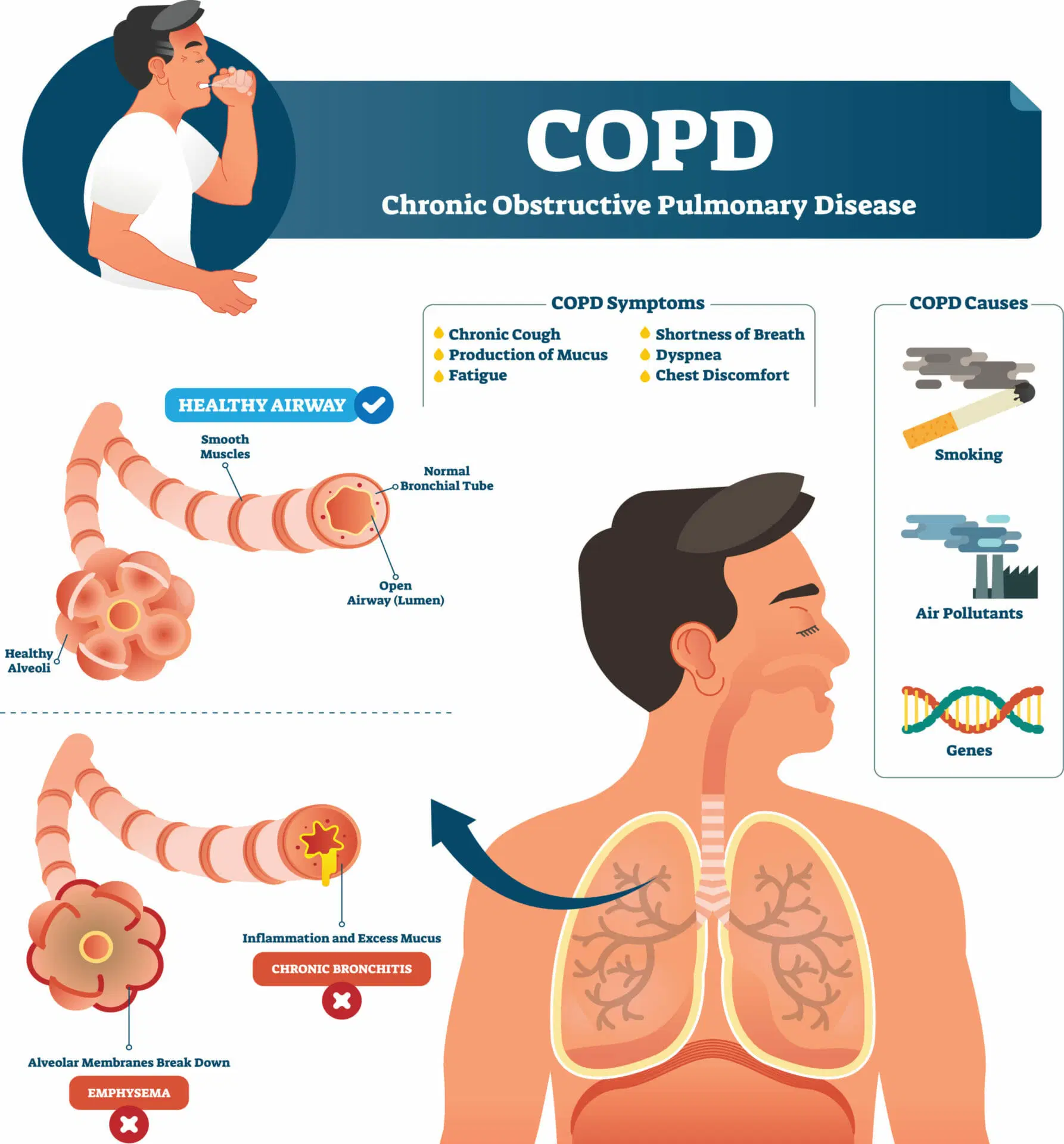
COPD is a chronic disease with several different causes. The most common cause is smoking because the lungs are subjected to chronic irritation of an inhaled substance 20 to 40 times each day for years on end. As a result, the lung tissue becomes inflamed. Under normal circumstances, body tissue is able to repair itself. However, in the case of smoking, chronic, repeated exposure to the irritants prevents healing and results in chronic inflammation. Over time, permanent damage occurs. The walls of the delicate alveolae lose their elasticity and become permanently distended, like balloons that have been inflated too many times. The walls of the alveolae also erode and thicken and, as a result, function less effectively. They begin to trap air rather than allow it to escape during expiration. This decreases the amount of oxygen-rich air that can be inhaled in each breath.
As chronic air-trapping occurs, the chest changes dimension, becoming more barrel-like. The lungs also flatten on the bottom, robbing the diaphragm (an important respiratory muscle) of its
effectiveness. Cilia in the airway normally move foreign debris upward to be coughed out. But in COPD, cilia become clogged with tar and lose effectiveness. As a result of these physical changes, the COPD patient may begin to experience some or all of the following symptoms:
orthopnea: The need to remain upright in order to breathe effectively. Physicians often quantify the severity of orthopnea by referring to the number of pillows the patient must recline against while sleeping (3-pillow orthopnea).
hypercapnia: The chronic retention of CO2. In some cases, this changes the way the person’s body determines when to breathe. The person may begin to function according to the “hypoxic drive” and feel the urge to breathe when the O2 level gets too low instead of when the CO2 level gets too high. This becomes a problem when the person requires supplemental O2. Too much O2 can, in some circumstances, actually knock out the urge to breathe, leading to respiratory arrest. Furthermore, hypercapnea can lead so symptoms of mental cloudiness and lethargy.
Chronic hypoxia: A chronic lack of oxygen. As gas exchange becomes less effective, breathing becomes more and more difficult. Eventually the person becomes dependent on oxygen. Yet, in the last stages of the disease, supplemental O2 is of little help. The person feels chronically short of breath and becomes severely dyspneic with the slightest exertion.
Case Study Questions
1. Upon admission, Mrs. Freiderick was:
a. Having chest pain
b. Very short of breath
c. Breaching very slowly
d. Unconscious
2. Mrs. Frederick had:
a. An increased ability to breathe in
b. A decreased ability to breathe in
c. An increased ability to breathe out
d. A decreased ability to breathe out
3. Ms. Frederick’s oxygen saturation level was:
a. Checked by pulse oximetry
b. At a normal level
c. Not known
d. Higher than normal
4. When listening so Mrs. Fredericks’s lungs, the physician heard:
a. Normal sounds of air movement
b. A somewhat musical sound caused by partial airway obstruction
c. A high – pitched upper airway sound that indicates airway obstruction
d. A Barking “seal-like” cough
5. Which of the following statements is true?
a. Mrs. Freiderick normally slept lying down
b. It is always safe to give high levels of oxygen to people with COPD
c. Supplemental O2 effectively relieves dyspnea in the final stages of COPD
d. Mrs. Freiderick’s chest cavity had most likely become more barrel-like in shape
6. Which of the following statements is correct?
a. Cilia continue to work effectively in people with late-stage COPD
b. The only cause of COPD is smoking
c. People with COPD tend to develop chronic O2 retention
d. Arterial blood was immediately drawn to analyze the levels of O2, CO2, and pH.
7. In a person with healthy lungs, the drive to breathe is stimulated by:
a. Low levels of oxygen
b. A drop in blood pH caused by high levels of CO2
c. A feeling of emptiness in the lungs
d. A neurological message sent from the brain to the lungs


